
The biopsychosocial injury model is defined as a framework that explains injury risk, recovery, and rehabilitation through the interaction of biological, psychological, and social factors. Psychiatrist George Engel introduced the model in 1977 as a direct challenge to the biomedical model, which treated injury and illness as purely physical events. The biopsychosocial approach recognizes that a torn ligament, a fear of reinjury, and a fractured team relationship all affect how fast and how fully an athlete recovers. Understanding this framework is the first step toward building a recovery plan that actually works.
What is the biopsychosocial injury model and its three domains?
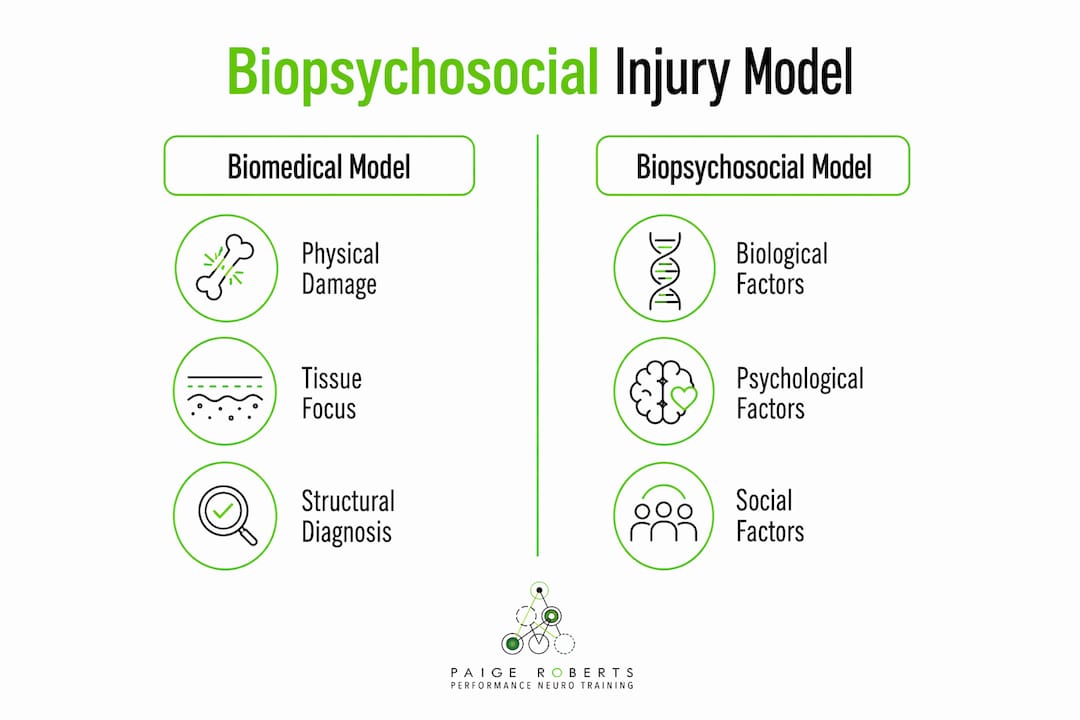
The biopsychosocial injury model integrates biological, psychological, and social factors into a single, unified picture of health. No domain operates in isolation. Each one shapes and is shaped by the others, which is what makes this framework so much more accurate than a purely physical diagnosis.
Biological factors
Biological factors include genetics, the physical injury itself, neurochemistry, sleep quality, and nutrition. A stress fracture is biological. So is the inflammatory response that follows it. Sleep deprivation slows tissue repair and raises cortisol, which directly extends recovery timelines. Nutrition deficits affect bone density and muscle regeneration. These are measurable, testable variables that form the physical foundation of any injury assessment.
Psychological factors
Psychological factors cover emotions, coping strategies, personality traits, and mental readiness. Personality traits like neuroticism increase susceptibility to injury and slow recovery. An athlete who catastrophizes pain will guard the injured area differently than one who approaches rehab with confidence. Fear of reinjury is one of the most documented barriers to return to play in sports medicine. These mental states are not soft variables. They produce measurable physiological changes in the nervous system.

Social factors
Social factors include relationships, team environment, social support, cultural expectations, and academic or work pressure. An athlete training under a coach who dismisses emotional distress faces a very different recovery environment than one with a psychologically safe team. Social load and academic pressure directly affect injury occurrence, not just recovery. The social environment either accelerates healing or quietly undermines it.
Pro Tip: Track your social load the same way you track your training load. If your relationships, work demands, and team stress are spiking, your injury risk is rising too.
How does the biopsychosocial approach improve assessment and treatment?
Moving from a purely biomedical diagnosis to a biopsychosocial formulation changes what clinicians look for and what they treat. A biomedical assessment asks: what is structurally damaged? A biopsychosocial assessment asks: what is limiting this person's activity, and what biological, psychological, and social factors are driving those limitations?
Clinicians using this framework follow a structured but flexible process:
- Assess activity limitations. The starting point is what the athlete cannot do, not just what the scan shows. Clinicians listen to patients' activity restrictions and link them to physical impairments and social consequences.
- Evaluate psychological readiness. Psychological readiness and self-reported function strongly predict return-to-play success. Clearing a physical threshold is not enough if the athlete's nervous system is still in threat mode.
- Map the social context. Work environment, team dynamics, and family support all influence healing speed. Patients share social context as scientific variables, not background noise.
- Build an interdisciplinary team. Effective biopsychosocial care requires collaboration among physical therapists, sports psychologists, physicians, and coaches. No single clinician can address all three domains alone.
- Reassess continuously. The formulation is not static. As biological healing progresses, psychological and social factors shift. The treatment plan must shift with them.
Chronic conditions like chronic pain respond far better to this approach. Interdisciplinary care addressing all three domains produces better outcomes than isolated physical treatment for conditions where the biomedical model alone falls short.
Pro Tip: Before your next rehab session, rate your stress level and sleep quality on a simple 1–10 scale. Share those numbers with your clinician. That data changes the treatment decision.
What evidence supports the biopsychosocial framework in sports injury?
The research base for this model in sports medicine has grown sharply. A 2024 systematic review confirmed that biopsychosocial factors affect both injury occurrence and recovery timelines. That finding matters because it shifts injury prevention from a purely physical training problem to a whole-person management challenge.
Predictive modeling now incorporates biopsychosocial variables. Researchers use regression, decision trees, and deep learning to forecast injury risk by combining sleep data, psychological scores, social load metrics, and physical history. These models outperform purely biomechanical predictors.
"No single factor causes injury or illness. It is the interaction of internal and external systems that the biopsychosocial model aims to capture." — The Center for Trauma and Stress Education
The table below shows how the biopsychosocial approach compares to the traditional biomedical model across key recovery dimensions.
| Dimension | Biomedical model | Biopsychosocial model |
|---|---|---|
| Diagnosis focus | Structural damage only | Activity limitations plus context |
| Treatment scope | Physical repair | Biological, psychological, and social domains |
| Return-to-play criteria | Physical clearance | Physical plus psychological readiness |
| Patient role | Passive recipient | Active partner in care |
| Outcome prediction | Imaging and physical tests | Multivariate biopsychosocial assessment |
The model also proves its value in complex cases. Conditions like chronic fatigue syndrome, Long Covid, and chronic pain require addressing all three domains to restore balance and reduce symptoms. Biomedical treatment alone consistently underperforms in these populations.
Understanding trauma-informed practices is one practical way sports professionals can begin applying this evidence in real settings.
What are common misconceptions about the biopsychosocial model?
Several persistent myths prevent athletes and clinicians from using this framework effectively.
- "Psychological factors are less real than physical ones." Fear of reinjury produces measurable changes in movement patterns and nervous system activation. Psychological factors are biological events expressed differently.
- "The model is a checklist." There is no set checklist. Clinicians build a formulation focused on structural inter-relationships, not a box-ticking exercise. Every athlete's picture is different.
- "Social factors are background context." Team psychological safety, coaching relationships, and family support directly alter recovery speed. They are treatment variables, not footnotes.
- "Addressing one domain is enough." Effective recovery requires simultaneous interventions across all three domains. Treating the knee without addressing the fear of reinjury or the hostile team environment produces incomplete results.
- "The model is too complex to use practically." Moving from biomedical to biopsychosocial care is genuinely challenging. The complexity is real. But the clinical insight it produces is worth the effort.
The biggest systemic barrier is entrenched biomedical thinking in clinical training programs. Many practitioners were trained to find and fix a physical cause. Shifting to a model that treats non-linear causality as the norm requires a different kind of clinical reasoning. Team psychological safety research shows that the social environment athletes train in is one of the most underaddressed variables in injury prevention.
Key Takeaways
The biopsychosocial injury model produces better recovery outcomes because it treats biological, psychological, and social factors as equally real and equally treatable.
| Point | Details |
|---|---|
| Three domains, one system | Biological, psychological, and social factors interact. Treating only one domain leaves the others unaddressed. |
| Psychological readiness matters | Self-reported function and mental readiness predict return-to-play success as strongly as physical clearance. |
| Social load drives injury risk | Academic pressure, team dynamics, and relationship stress raise injury occurrence, not just recovery time. |
| No checklist exists | Clinicians build individual formulations based on activity limitations and inter-relationships, not fixed protocols. |
| Interdisciplinary care is required | No single practitioner covers all three domains. Effective care requires collaboration across specialties. |
Why I think most injury recovery plans are still missing the point
Athletes come to me after months of physical rehab that technically worked. The tissue healed. The scans looked clean. But they still could not perform. They froze at the moment of competition or pulled back instinctively before contact. That is not a physical problem. That is a nervous system still running a threat response from an injury the body has already repaired.
The biopsychosocial framework explains exactly why this happens. The psychological and social domains did not get treated. The fear was never addressed. The team environment that made the original injury worse was never examined. Physical clearance was treated as the finish line when it was actually just the starting gate.
What I have found working with athletes at every level, including Olympic medalists, is that the nervous system holds the injury long after the tissue heals. Mental reprogramming after injury is not optional. It is the part of recovery that determines whether an athlete gets back to their previous level or plateaus just below it.
The biopsychosocial model gives clinicians and athletes a shared language for that reality. My work with Alpha Imprinting at Robertsneurotraining targets the nervous system directly, addressing the psychological and biological overlap that standard rehab programs skip entirely. The athletes who engage fully with all three domains of their recovery do not just return to play. They return better.
— Paige
How Robertsneurotraining supports your full recovery
Robertsneurotraining, led by Dr. Paige Roberts, applies neuroscience-based methods to address the psychological and biological dimensions of sports injury recovery. The program uses Alpha Imprinting to reprogram the nervous system, clearing the mental blocks and threat responses that standard physical rehab leaves behind. If you are ready to address all three domains of your recovery, the Energy Optimization Workbook is a practical starting point for understanding how your nervous system is affecting your performance. For a deeper look at the full process, explore the neurotraining process and see how biopsychosocial principles are built into every step.
FAQ
What is the biopsychosocial injury model in simple terms?
The biopsychosocial injury model is a framework that explains injury and recovery through three interacting factors: biological (physical damage, genetics, sleep), psychological (emotions, fear, coping), and social (relationships, team environment, cultural pressure). No single factor causes injury alone.
How does the biopsychosocial model differ from the biomedical model?
The biomedical model focuses only on physical causes and structural damage. The biopsychosocial model adds psychological readiness and social context as equally important variables in both diagnosis and treatment.
What psychological factors affect sports injury recovery?
Fear of reinjury, neuroticism, low psychological readiness, and poor coping strategies all slow recovery and reduce return-to-play success rates. Psychological readiness is now considered a key criterion for return-to-play decisions alongside physical clearance.
Can social factors really cause a sports injury?
Yes. Research confirms that social load, academic pressure, and poor team environments raise injury occurrence directly, not just recovery time. Managing social stress is a legitimate injury prevention strategy.
How do clinicians apply the biopsychosocial framework in practice?
Clinicians build individual formulations by assessing activity limitations, mapping psychological readiness, and evaluating social context. The process is not a checklist. It focuses on the inter-relationships between all three domains to guide treatment decisions.